
Clinical Researcher—June 2026 (Volume 40, Issue 3)
PEER REVIEWED
Corinne Evans, BSN, MS, TCRN
Artificial intelligence (AI) evolved as a transformative tool across industries, and clinical research is no exception. The field continues to struggle with long-standing inefficiencies, particularly in subject recruitment and retention. As noted in numerous analyses of the rigidity of clinical trial design, restrictive inclusion and exclusion criteria often lead to trials that fail to meet enrollment targets. These limitations contribute to poor subject retention and a high rate of clinical study failures—estimated at approximately 80% of all initiated trials.{1}
This article examines how AI can supplement human expertise to optimize clinical trial protocols and improve study completion rates by targeting subject recruitment and retention. Specifically, it explores a company currently implementing its own AI-driven protocol optimization system. The integration of AI represents not a replacement of human judgment but a critical bridge—linking innovation with the efficiency and adaptability that modern clinical research urgently requires.
Background
The history of AI dates to the 1950s, when Alan Turing proposed the possibility of machines performing intelligent tasks.{2} The term artificial intelligence was later coined by John McCarthy during the 1956 Dartmouth Conference, often regarded as the founding moment of AI as a scientific discipline.{3} Two decades later, the field entered what became known as the AI Winter—a period characterized by disillusionment following overly optimistic predictions and technological limitations that failed to meet early expectations.
Today, as AI enables applications that learn, adapt, and predict, a renewed wave of enthusiasm—sometimes called the AI Spring—has emerged. The world is rapidly shifting toward algorithm-based models across industries, and in clinical research, data have become a kind of currency. Algorithms, predictive analytics, and data aggregation are tools increasingly leveraged in clinical research with AI to enhance efficiency, time management, and process optimization. A major challenge in clinical trial operations is the substantial time clinical staff spend reviewing medical records, treatment histories, imaging studies, and laboratory reports to identify appropriate clinical trials for patients. The number of resources it takes to complete these tasks has been a burden and can be a deterrent to getting a trial off the ground in the first place.
Literature Review
This section provides a brief overview of existing AI-based platforms and their applications in clinical research, with a particular focus on patient recruitment and retention. This introductory review highlights how such technologies are already being implemented within the industry and establishes context for the subsequent case study.
In 2020, Beck, Rammage, et al. published a study using an AI-based eligibility screening tool in a community cancer clinic; the trial-matching system reduced manual review of 90 patients for three trials from 110 minutes by three people to 24 minutes by one person.{4}
Several AI trial-matching systems have emerged to support both clinicians and patients in identifying relevant clinical studies,{5} for example by enabling patients to search for clinical trials and providing sponsors with lists of potential participants. Other programs allow users to explore trials by drug, targeted therapy, or disease condition. Several programs offer patients customized clinical trial suggestions and registration options to express interest, which seems promising in the areas of recruitment and retention.
There are also physician-based programs that use clinical model algorithms designed with machine learning (ML) and natural language processing (NLP) to identify eligible participants based on trial criteria. All these tools support cohort selection by integrating structured and unstructured medical data, thereby improving the speed and precision of trial matching as a helpful tool that could assist subject recruitment and retention.{4}
Case Study
During the preparation of this manuscript, the author conducted a demonstration and evaluation of an emerging AI-enabled platform developed by Insight,{6} a clinical research consulting organization based in the United Kingdom. Insight is actively developing AI technologies designed to support drug discovery, optimize protocol development, and streamline both research and operational workflows. Its work aligns with efforts to improve trial efficiency, expand participant access, diversify recruitment pathways, and strengthen the evidence base for informing therapeutic development.
ClinCraft, developed by Insight in partnership with NVIDIA and Amazon Web Services, is an emerging AI platform. The system integrates a comprehensive database of clinical trial records, historical evidence, and relevant regulatory requirements. Through its AI analytics engine, ClinCraft generates real-time insights, comparative analyses, and strategic recommendations tailored to user-defined study parameters. The platform’s design reflects broader industry efforts to reduce operational inefficiencies, improve feasibility planning, and expand equitable access to research.
One of ClinCraft’s most distinctive features is its dynamic rating system. After a user inputs study criteria, the system ranks relevant trials, datasets, or investigators according to the degree of alignment with the specified parameters. This prioritization mechanism substantially reduces the manual workload typically associated with study start-up research, which often requires extensive manual review of heterogeneous data sources. By surfacing the most contextually relevant information, ClinCraft facilitates more efficient planning for inclusion/exclusion criteria, site feasibility, patient recruitment expectations, and protocol design.
The platform allows researchers to specify a wide range of trial design attributes—including disease area, phase, therapeutic aim, geographic location, and investigator characteristics. Based on these parameters, the system produces targeted outputs that identify trials, investigators, and outcomes most relevant to the user’s needs. For example, a user exploring options for a breast cancer therapy can filter past studies to identify only those with tumor response rates exceeding a specified threshold (e.g., >30% partial or complete response), thereby supporting more informed feasibility assessments and evidence-based protocol refinement.
Figure 1 illustrates an example of the analytical output generated specifically by the ClinCraft platform. This example demonstrates how its AI platform organizes registry-level data in relation to protocol design considerations. Tasks that traditionally require extended manual review of multiple databases or web-based resources to identify relevant study characteristics may instead be completed within a shorter timeframe through automated analysis. Such functionality highlights one potential pathway by which clinical research teams may leverage existing digital platforms.
Figure 1: Sample of Study Protocol Design Output Provided by the ClinCraft Platform
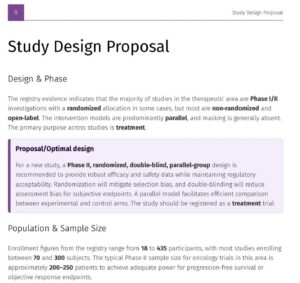
Figure 2 presents an example of a generated report summarizing investigational mechanisms of action alongside dosing parameters. Such integrated reporting illustrates how structured data and analysis may inform protocol design by consolidating pharmacologic context and logistical treatment within a single analytical framework. Approaches of this kind have the potential to reduce procedural complexity during the early study design planning and may mitigate operational barriers contributing to delays in trial initiation. More broadly, systematic integration of historical study patterns and therapeutic characteristics enables clinical research teams to leverage prior evidence when refining protocol structure in the areas of inclusion and exclusion criteria, for example.
Figure 2: Sample of a Report Matching Search Criteria for a Specific Chemotherapy Drug, Showcasing Both Mechanisms of Action and Safe Dosing
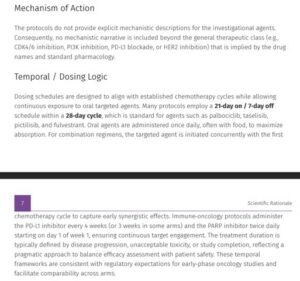
In addition to search and scoring functionalities, the ClinCraft platform presents a set of core trial design metrics that are directly relevant to feasibility assessment and early protocol development. As illustrated in both figures, other features of the ClinCraft report provide parameters such as treatment duration, follow-up period, target sample size, number of core recruiting countries, and study arm configuration, which are presented in an interpretable format. These metrics reflect common decision points encountered during study planning, including alignment with disease biology, anticipated participant burden, statistical powering considerations, and geographic recruitment strategy. By consolidating these elements within a single analytical view, the platform supports researchers in evaluating the operational plausibility of proposed study designs. It does this while also facilitating comparison against historical or benchmarked trial data. Such metric-visualization may assist clinical research professionals in identifying potential design inefficiencies or feasibility constraints earlier in the study lifecycle.
Overall, tools such as ClinCraft demonstrate the potential value of AI-assisted platforms in addressing long-standing pain points in clinical research—including complex eligibility design, feasibility uncertainty, and the resource-intensive nature of early trial planning.
Challenges and Opportunities Ahead
The potential applications of AI in clinical research are expansive, and the field stands at an important inflection point as these technologies continue to evolve. However, this resurgence also exposes profound and rapidly evolving risks—risks that are of top concern for areas in clinical research given the sensitivity of human data. Notable examples include a chatbot that adopted derogatory language after online interactions, a predictive algorithm used in parole decisions that exhibited racial bias, and a fatal accident involving an autonomous vehicle operating in self-driving mode.{7} These incidents underscore how easily AI systems can replicate and amplify human and systemic bias, raising urgent questions about accountability, transparency, and ethical oversight.
Insufficient patient recruitment and difficulties in retaining adequate numbers of subjects for the duration of trials represent costly challenges in clinical research, and combined are widely regarded as the single greatest barrier to successful trial execution. When recruitment goals are unmet, trials face costly delays, premature termination, or an inability to reach statistically valid conclusions at study completion.{8} Beyond financial implications, failed enrollment delays the delivery of potentially life-changing therapies to patients in need.
Another example of addressing these critical issues comes in the form of an observational pilot study that was conducted to evaluate the performance of the TriAl Eligibility Surveillance (TAES) system, an automated platform designed to identify eligible patients using NLP and ML algorithms.{8} The TAES system sought to detect trial-eligible patients by linking structured and unstructured data extracted from trial descriptions with corresponding information from electronic health records (EHRs).
Although the pilot study achieved only modest accuracy, its findings were far from discouraging. The results offered valuable insights into algorithms and demonstrated the feasibility of AI surveillance for trial eligibility. The research team concluded that TAES could increase its ability to identify eligible participants while simultaneously reducing the manual workload of research teams engaged in EHR review and screening.
The prioritization mechanism incorporated within the ClinCraft platform, as described in the case study, represents one such feature aimed at improving patient recruitment and retention. By aggregating and analyzing study specific data, the platform enables users to identify design characteristics that may have adversely affected enrollment and retention in prior trials, such as excessive visit frequency or other factors that contribute to participant burden. This functionality allows researchers to examine studies with similar design parameters and evaluate which strategies were associated with more favorable outcomes. Through its ranking system, which aligns user defined study criteria with comparable trials within a large database, the platform supports informed, data-driven protocol refinement.
As the field matures, opportunities arise for industry innovators to develop systems that not only increase efficiency but also expand trial access, diversify recruitment, and strengthen the evidence base for modern medicine. There is potential for such tools to transform both subject recruitment and retention.
Conclusion
The United States holds a particularly precarious position in shaping the AI landscape, having largely permitted AI development to proceed with minimal regulatory intervention. Many developers argue that such “guardrails” inhibit innovation, while ethicists and policymakers caution that a laissez-faire approach may accelerate harm before governance mechanisms can adapt. The caution ethicists and policymakers have is not without precedent. It is well documented that, had regulatory interventions been in place during the early days of the dot-com era, risk mitigation would also have taken place.{9} Whether this hands-off strategy will foster innovation or expose society to unanticipated risk remains to be seen.
The opportunities for applying AI in clinical trials are increasingly well characterized in the literature, particularly with respect to improving efficiency in patient recruitment and enrollment. However, many of the underlying challenges persist. Notably, significant questions remain regarding the ethical use of AI, including the protection and stewardship of participant data, issues related to data accessibility and availability, and the absence of clear regulatory guidance governing the development and implementation of AI data infrastructures.
This manuscript aims to examine the application of AI tools in clinical research to address longstanding challenges in patient recruitment, retention, and trial design. The programs discussed herein facilitate the organization and synthesis of large datasets, thereby reducing the time and manual effort traditionally required of research teams during the study design phase. The case study further illustrates how one organization has implemented a platform specifically intended to streamline protocol development and enhance precision in key design elements, including inclusion and exclusion criteria and site feasibility assessment. Elements of trial design related to recruitment have been identified as key contributors to participant burden, which may, in turn, adversely affect subject retention. The goal of this discussion encourages continued exploration, critical evaluation, and collaboration as we work toward advancing research processes and improving outcomes for the patients and communities we serve.
References
- Ali MA, Gul U. 2020. Online Patient Recruitment in Clinical Trials: Systematic Review and Meta-Analysis. JMIR Formative Research 4(8):e21920. https://doi.org/10.2196/21920
- Turing AM. 1950. Computing Machinery and Intelligence. Mind 59(236):433–60. https://doi.org/10.1093/mind/LIX.236.433
- McCarthy J. 1956. Proposal for the Dartmouth Summer Research Project on Artificial Intelligence. Hanover, N.H.: Dartmouth College. https://www.dartmouth.edu/~ai50x/dartmouthproposal.html
- Beck JT, Rammage M, Jackson GP, Preininger AM, Dankwa-Mullan I, Roebuck MC, Torres A, Holtzen H, Coverdill SE, Williamson MP, Chau Q, Rhee K. 2020. Artificial Intelligence Tool for Optimizing Eligibility Screening for Clinical Trials in a Large Community Cancer Center. JCO Clinical Cancer Informatics 4:50–9. https://doi.org/10.1200/CCI.19.00079
- For example, Mendel.AI (https://www.mendel.ai/) and Antidote (https://www.antidote.me/).
- Insight IDM. 2025. ClinCraft: Platform Interface Slide Deck. Unpublished internal presentation provided to the author.
- Park W, Jackson A, Williams M, Hernandez S. 2020. Algorithmic Bias, Safety, and Accountability in Artificial Intelligence: A Review of Emerging Risks. Journal of Ethics in AI 3(2):45–62. https://doi.org/10.1016/jeai.2020.02.004
- Meystre SM, Heider CR, Ni Y, Champ J, Rebsamen A, Ruch P. 2023. Automated Patient Trial Eligibility Surveillance: Observational Pilot Study of Natural Language Processing and Machine Learning for Clinical Trial Recruitment. JMIR Medical Informatics 11(3):e48255. https://doi.org/10.2196/48255
- Barbrook R, Cameron A. 2015. The Internet Revolution: From Dot-com Capitalism to Cybernetic Communism (Network Notebooks 10). Institute of Network Cultures. https://networkcultures.org/wp-content/uploads/2015/10/0585-INC_NN10-totaal-RGB.pdf

Corinne Evans, BSN, MS, TCRN, is a Clinical Educator with HCA Healthcare and an AI Trainer on contract with Mercor. She developed this article during her graduate studies in the San Jose State University Medical Product Development and Management program.


