
Clinical Researcher—August 2024 (Volume 38, Issue 4)
PRESCRIPTIONS FOR BUSINESS
Sam Srivastava
One of the biggest challenges facing the clinical research industry now is lack of stakeholder engagement. Trials are increasingly complex: taking longer, costing more, and requiring more technology and data than ever. It took an average of 7.1 years to develop a new drug (from starting clinical trials to approval) in 2022 (up from 6.9 years in 2021) at an average cost of $2.3 billion, according to the Deloitte Centre for Health Solutions.{1} A clinical investigator at a hospital or in a doctor’s office trying to manage a trial now uses more than 12 pieces of technology, on average.{2}
For people who want to participate in a clinical trial, the barriers are high. They must first overcome the fact that only 3% of physicians globally participate in clinical trials, so their doctor probably isn’t involved.{3} Then, if they do find a pertinent clinical trial, 70% of people must drive an average of more than two hours to participate.{4} Furthermore, they must change their pattern of care to go to the clinical research site. It’s very burdensome, and just one of the reasons contributing to the fact that more than 30% of participants in a trial drop out over time.{5}
Personal Perspective
Unfortunately, my father had amyotrophic lateral sclerosis (ALS) and passed away from the disease. I spent much of my time working with payers, providers, social workers, and employers trying to get a better system of care for my father. Now, I’m fortunate to be in a position of helping sponsors determine how to cure ALS, working in an organization involved in everything from trial design, start-up, and partnering with sites to recruiting patients, gathering clinical endpoints, and completing a trial.
However, as I took on this job, I quickly discovered that the clinical research delivery model is even more antiquated than the care delivery system. For the past 10 years, the care delivery system has been aligning around value-based access, affordability, quality, and experience. Clinical research has a terrific opportunity to rally around that same quadruple aim.
Improving Access and Affordability
We need to make it easier for people to participate in clinical research. The strategies employed to connect patients with clinical research sites also need to vary by geography. There are distinct differences between urban, suburban, and rural communities. Successful outreach requires cultural competency, knowledge of how care is delivered, and attention paid to how research is understood in local markets. It’s not just the language that information is written in, but also the cultural sensitivities that are critically important.
We have an elegant process for capturing data and identifying participants who might be eligible for a trial, running their information against inclusion and exclusion criteria, understanding the sites and their ability to perform, and figuring out which ones might be suitable for a trial. The bigger challenge is reaching out to those potential participants—enabling them, and sometimes their family members, to better understand the trial. This would help them enroll, while ensuring they have transportation to and from the research site will help them to stay enrolled.
We talk about social determinants of care as barriers to care delivery, but there are also social determinants to clinical research. On average, 75% of the U.S. participants in clinical trials are white Caucasians. That does not reflect the United States, where approximately 40% of the population is multiethnic and diverse.{6}
We tend to conduct clinical research where participants have means and awareness, so they’re typically white, affluent, educated, and in urban settings. From an ethical perspective, we need to do better at reaching into communities and personalizing clinical trials so that the social determinants of clinical research are effectively addressed.
Improving Quality and Experience
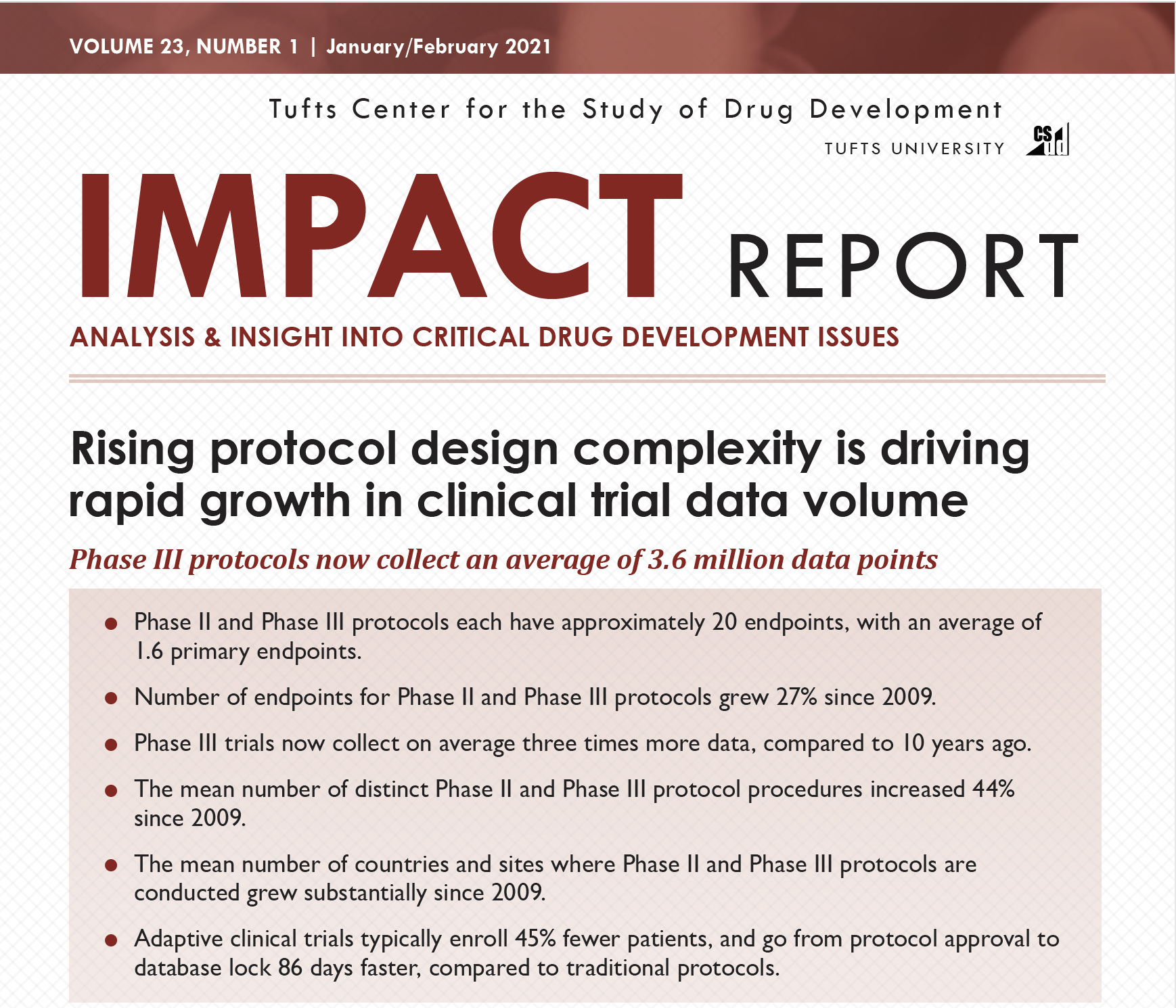
The data required for a clinical trial, and the evidence that’s generated and collected, is three times greater than 10 years ago.{7} As an industry, we have a great opportunity to improve the quality and efficiency of data collection and use now.
One step in the right direction is for organizations to host external advisory committees—ideally composed of leading industry experts from all stakeholder groups—so that new perspectives can help organizational leaders be ready for the challenges on the horizon relevant to the interaction of care and trials, in terms of patient centricity and transparency, among other concerns. Underscoring the importance of this type of engagement, research conducted by the Tufts Center for the Study of Drug Development showed that protocols which were developed with a patient advisory board had a 30% reduction in clinical endpoints, 20% fewer inclusion/exclusion criteria, and a 50% reduction in the amount of data collected, significantly simplifying the trials.{8}
Innovation is central to the ability to accelerate clinical research, which is why more organizations should also host “innovation studios” to allow scientists, managers, clinicians, and product and technology leaders to come together to focus on big, bold technology and product innovations. Such studios allow organizations to take an idea, develop it, test it, and have a viable product or service that is delivered to the market at warp speed. For example, in one organizational setting, an innovation studio-inspired approach to streamlining operational processes has allowed institutional review board services that used to take 45 days to conduct to be reduced to an average of four or five days.{9}
Industry Call to Action
As an industry, we have not been able to bring care delivery into alignment with clinical research; however, we have a powerful opportunity to see this through now with the confluence of data and technology, backed by a drive to make clinical trials more diverse and personalized.
Let’s bring the quadruple aim in care delivery to clinical research. Let’s start with the patient and make clinical research more accessible, more affordable, higher quality, and a better experience. Let’s make the system better for everybody—not incrementally or in just a few small ways, but by rapidly and fundamentally reinventing it.
Next Steps
We can start by building coalitions of all the stakeholders—sites, sponsors, contract research organizations, regulators, vendors, and more—and publicizing collaborations that have produced great outcomes by sharing best practices and tools that are leveraged as a group.
Second, we can work with leaders at global forums to make this agenda item number one.
Third, we need to get grassroots, community-based organizations and regulatory authorities involved.
Overall, we need to demonstrate proof of concept and the will and support around it to move from quality issues toward this call to action wrapped around access, affordability, quality, and experience.
Finding ways to break down barriers, drive interoperability, and increase connectivity will enable fresh thinking and collaborative approaches that will help to make the quadruple aim a reality for clinical research.
References
- Deloitte Centre for Health Solutions. 2023. Seize the digital momentum: Measuring the return from pharmaceutical innovation 2022. https://www2.deloitte.com/ch/en/pages/press-releases/articles/deloitte-pharma-study-drop-off-in-returns-on-r-and-d-investments-sharp-decline-in-peak-sales-per-asset.html
- Carozza D. 2020. Tool or Bludgeon: Technology Can Support Clinical Trial Sites or Undermine Them. How Are You Using It? Clinical Researcher 34(3). https://acrpnet.org/2020/03/10/tool-or-bludgeon-technology-can-support-clinical-trial-sites-or-undermine-them-how-are-you-using-it
- WCG. 2023. Trust Between Participants and Sites Starts with Engagement. https://www.wcgclinical.com/insights/trust-between-participants-and-sites-starts-with-engagement/
- Deloitte. 2022. Broadening clinical trial participation to improve health equity. https://www2.deloitte.com/us/en/insights/industry/health-care/increasing-diversity-clinical-trials.html
- National Library of Medicine. 2013. The Uphill Path to Successful Clinical Trials. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3684189/
- United States Census Bureau. 2021. Improved Race and Ethnicity Measures Reveal U.S. Population is Much More Multiracial. https://www.census.gov/library/stories/2021/08/improved-race-ethnicity-measures-reveal-united-states-population-much-more-multiracial.html
- Tufts Center for the Study of Drug Development. 2021. Rising protocol design complexity is driving rapid growth in clinical trial data volume. https://f.hubspotusercontent10.net/hubfs/9468915/TuftsCSDD_June2021/images/Jan-Feb-2021.png
- CenterWatch. 2023. Patient Advisory Boards Essential to Mitigating Protocol Complexity, Experts Say.
https://www.centerwatch.comhttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC3684189/ /articles/26615-patient-advisory-boards-essential-to-mitigating-protocol-complexity-experts-say - National Library of Medicine. 2017. Time to institutional review board approval with local versus central review in a multicenter pragmatic trial.
https://pubmed.ncbi.nlm.nih.gov/28982261/
 Sam Srivastava is Chief Executive Officer of WCG.
Sam Srivastava is Chief Executive Officer of WCG.



{kind=link}