
Clinical Researcher—June 2026 (Volume 40, Issue 3)
PEER REVIEWED
Justin Scott Brathwaite, MBA, PMP; Syed A. A. Rizvi, MD, PhD(Pharm), PhD(Chem), MPH, MBA, MS, MSN, MSc, BSc, BSN, CCRN, CEN, CMRN, TNS, VA-BC, LSSBB, FRSM
Artificial intelligence (AI) is rapidly transforming clinical research, yet its successful adoption depends on aligning technological innovation with workforce readiness and site-level realities. This article applies the Technology Acceptance Model (TAM) as a theoretical foundation to examine how clinical research coordinators (CRCs) and clinical research associates (CRAs) perceive the integration of AI into their workflows. It also examines the role of AI literacy as a determinant of preparedness for technology-driven workflows.
The AI Literacy Questionnaire (AILQ), a validated instrument measuring affective, behavioral, cognitive, and ethical dimensions of literacy, is proposed to assess baseline knowledge and inform workforce development strategies. By pairing TAM with site-centric industry practices, this framework emphasizes the importance of human-centered design, validated assessment tools, and practical implementation strategies. Together, these insights offer an evidence-based approach for advancing sustainable, ethical, and effective AI adoption within clinical research operations.
Background
AI is rapidly reshaping clinical research, offering unprecedented opportunities to enhance efficiency, accuracy, and patient engagement. Yet, the success of AI integration depends not solely on the technology itself, but also on the competency and perceptions of those tasked with utilizing it in their workflows. Although clinical research professionals, including CRCs and CRAs, are vital to the successful execution of clinical trials, their perspectives on AI adoption and literacy, as well as their baseline competencies, remain underexplored.
The successful integration of AI into clinical research workflows depends less on the technology itself and more on the people who will use it. User acceptance, confidence, and practical competence, often described collectively as AI literacy, play a central role in whether AI tools are adopted effectively in real-world research settings. One practical way to address this is to ground implementation efforts in established frameworks, such as TAM, and to assess AI literacy using validated survey instruments periodically. These approaches help clarify how clinical research professionals perceive AI, how much they trust it, and how comfortably they incorporate it into daily practice.
This issue is significant because current regulatory guidance offers limited direction on how AI should be operationally embedded into clinical research workflows. The U.S. Food and Drug Administration’s (FDA’s) January 2025 draft guidance focuses primarily on situations in which AI-generated outputs are used to support regulatory decisions related to drug safety, effectiveness, or product quality. By contrast, AI applications used internally, for example to assist with study planning, document drafting, or resource allocation, generally fall outside FDA oversight unless they directly affect patient safety or data integrity.{1}
When AI systems do influence clinical or research decisions, such as determining patient eligibility, generating endpoints, monitoring safety signals, or informing dose selection, the FDA expects sponsors to define the model’s intended context of use clearly and to evaluate risk based on both the level of influence and the potential consequences of error.{1} In these cases, emphasis is placed on transparency, data quality, bias mitigation, uncertainty management, and appropriate documentation. Notably, however, decisions regarding governance structures, workforce training, and day-to-day operational implementation are primarily left to sponsors and institutions.
For this reason, meeting regulatory expectations alone is not sufficient to ensure successful AI adoption. Meaningful and sustainable use of AI in clinical research requires parallel investment in workforce preparedness, ongoing education, and thoughtful change management to bridge the gap between regulatory compliance and practical implementation.
Therefore, as the industry continues to adopt more site-centric models that emphasize workflow optimization, it becomes essential to understand how frontline professionals perceive, accept, and prepare for AI-enabled tools. This article applies the TAM as a theoretical foundation to examine these dimensions and proposes structured research questions for further investigation. Moreover, it also argues for assessing baseline AI literacy among clinical research professionals using validated survey tools to guide evidence-based, human-centered strategies for sustainable innovation in clinical research. Lastly, the article provides recommendations for industry stakeholders to implement AI technologies within their organizations.
Understanding the Knowledge Gap in AI Adoption Within Clinical Research
AI has emerged as an incredibly transformative technology within clinical development, with the potential to improve trial efficiency, streamline data management, and reduce administrative burdens.{2,3} However, despite its promise, our understanding of how AI is being implemented, or could be implemented within clinical research workflows, is ongoing. Most significantly, our review of the existing literature provides sparse information assessing the operational and human factors of AI adoption among site-level research personnel. More specifically, studies evaluating the viewpoints and baseline AI knowledge of CRCs and CRAs are markedly absent.
These roles are central to both site operations and oversight, acting as the bridge between sponsors, investigators, and participants.{4,5} Moreover, their experiences determine whether technologies like AI are seamlessly integrated or met with resistance. Yet these professionals’ perspectives remain largely unexamined within the context of AI implementation. This gap constrains efforts to foresee and address challenges associated with AI workflow integration and staff training, both of which are essential for long-term, sustainable adoption.
This knowledge deficit also has broader implications for workforce sustainability, particularly in an industry already facing high rates of burnout, turnover, and operational strain.{6} Without a clear understanding of how AI affects the day-to-day responsibilities of research staff or the competencies required for its use, its potential benefits for the workforce may not be fully realized.
Addressing these questions will move the field beyond anecdotal claims, providing the empirical foundation necessary to ensure AI can truly mitigate site-level burdens, enhance data quality, and support personnel retention.
To guide this exploration, the TAM provides a well-established theoretical framework. By examining how its core constructs perceived usefulness, ease of use, and behavioral intention influence technology adoption, the TAM helps frame research questions and hypotheses that illuminate the human dimensions of AI integration in clinical research.{7} Moreover, effective implementation begins with assessing baseline AI competencies among research staff using validated surveys, ensuring that workforce readiness aligns with technological advancement.
Linking Theory to Inquiry: Using the TAM to Generate Research Questions on AI Adoption
The TAM, developed by Fred Davis in 1989, is one of the most influential frameworks for understanding how users adopt and utilize new technologies. Grounded in the Theory of Reasoned Action, TAM posits that two primary beliefs drive technology adoption: perceived usefulness (PU) and perceived ease of use (PEOU). PU refers to the degree to which an individual believes that using technology will enhance their job performance, while PEOU refers to how effortless they perceive the technology to be. These two factors influence a person’s attitude toward using the system, which in turn shapes their behavioral intention to use it, ultimately predicting actual system use.{8}
Over time, several updates have refined the original model. TAM2 incorporated social and cognitive factors like subjective norms, image, and job relevance, recognizing that organizational and peer influences play a role in technology acceptance.{9} TAM3 further expanded on these ideas by integrating determinants of PEOU, such as computer self-efficacy, perceived enjoyment, and anxiety, providing a more comprehensive view of how both individual differences and system characteristics affect acceptance.{10}
In practice, the TAM has been widely applied across fields such as healthcare, education, and business to assess how individuals respond to innovations like electronic health records, AI systems, or digital learning tools.{11} In clinical research, the TAM could help explain how staff adopt AI platforms for tasks such as patient recruitment and trial monitoring. When users perceive these tools as improving efficiency (high PU) and being easy to use (high PEOU), they are more likely to accept and integrate them into their workflows.
Application of the TAM Theoretical Framework to Clinical Research Operations
A critical question that can be examined through the TAM is how clinical research professionals perceive the integration of AI within patient recruitment and retention. The TAM enables investigators to examine how end-users interpret the value and usability of AI within a domain that remains both operationally demanding and underexplored.
While enthusiasm for AI in clinical trials continues to grow, implementation strategies have primarily been shaped at the organizational level, highlighting an opportunity to incorporate more insights from frontline research professionals.{12} Consequently, there is a persistent gap in understanding how research staff conceptualize AI’s potential benefits, challenges, and alignment with real-world workflows. Without systematically capturing these perceptions, organizations risk developing AI tools that fail to address site-level realities, thereby reinforcing inefficiencies or generating user resistance outcomes that directly influence the attitude toward use component of the TAM and ultimately determine whether adoption efforts succeed or fail.
To address this gap and align with the needs of the clinical research industry, the following sub-questions can be examined in accordance with the core domains of the TAM using structured questionnaires. The integration of the TAM and Diffusion of Innovations models provides a conceptual lens to understand adoption behavior (see Table 1).
Table 1: Linking the TAM Constructs to Research Questions—Exploring AI Adoption Among Clinical Research Professionals
| TAM Domain | Potential Area of Inquiry |
| Perceived Usefulness | How do CRCs and CRAs perceive the usefulness of AI tools in improving efficiency, accuracy, and outcomes in patient recruitment and retention? |
| Perceived Ease of Use | To what extent do they believe these systems will be easy to learn, operate, and integrate into workflows? |
| Attitude Toward Use | What are their prevailing attitudes regarding trust, ethical concerns, and the impact on patient relationships? |
| Behavioral Intention to Use | What is the likelihood that they would adopt or recommend AI tools if available and aligned with their professional needs? |
Assessing AI Literacy and Workforce Preparedness Among Clinical Research Professionals
Alongside understanding perceptions of AI adoption through the TAM, it is equally important to assess the baseline level of AI literacy among clinical research staff to inform the design of targeted educational programs that support workforce development. These initiatives would provide value not only to professional organizations such as the Association of Clinical Research Professionals (ACRP) and the Society of Clinical Research Associates (SOCRA), which prioritize workforce development, but also to industry stakeholders invested in strengthening site capacity and operational efficiency.
A critical question emerging from this discussion is: What is the baseline level of AI literacy among clinical research professionals, including CRCs and CRAs, and how can this understanding inform the design of targeted educational interventions to support AI integration in clinical research workflows? This question centers on AI literacy and workforce preparedness, focusing on CRCs and CRAs who are directly responsible for the daily execution, monitoring, and documentation of clinical trials.
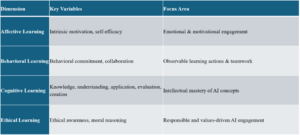
To address this issue, the AILQ, a validated and emerging instrument measuring affective, behavioral, cognitive, and ethical dimensions of AI literacy, offers a structured means of evaluating current knowledge.{13} Findings derived from the AILQ can help identify training needs and inform the design of evidence-based educational programs that strengthen AI readiness across the clinical research workforce (see Table 2).
Table 2: Elements of the AI Literacy Questionnaire
Grounding Research in Theory and Site-Centric Practice
The previously outlined research questions, grounded in the TAM and supported by validated survey tools, should be considered alongside industry practices that have demonstrated effectiveness, such as the site-centric approach.{14} Increasingly, contract research organizations and sponsors are adopting site-centric strategies to enhance collaboration and improve the site experience.{14–16} This philosophy emphasizes understanding and addressing the needs and operational challenges of research sites when designing systems and workflows.
Pairing validated theoretical frameworks like the TAM with established industry practices provides a strong foundation for studying and guiding AI adoption. In this context, being site-centric extends beyond improving communication; it involves leveraging AI to streamline operations, reduce administrative burden, and supporting workforce retention. Achieving these goals requires the use of validated instruments to accurately capture research staff perceptions and operational barriers. Integrating theoretical rigor with practical, site-centered strategies offers a balanced, evidence-based approach to ensuring that AI solutions are both effective and sustainable in clinical research.
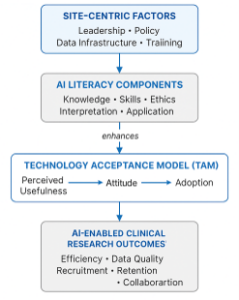
As illustrated in Figure 1, the integration of AI literacy with the TAM constructs provides a framework for understanding adoption behavior among clinical research staff.
Figure 1: Conceptual Framework Integrating AI Literacy, the TAM, and Site-Centric Implementation for AI Adoption in Clinical Research
Key Takeaways for Clinical Research Stakeholders
For AI-driven platforms to achieve meaningful adoption and deliver practical value, several guiding principles should be considered. These principles provide a framework for aligning innovation with operational needs while emphasizing human-centered design, workforce preparedness, and ethical responsibility. By incorporating these considerations early in development, industry professionals can help ensure that AI implementation complements existing site operations, enhances efficiency where appropriate, and supports long-term sustainability within the clinical research ecosystem.
CRCs and site staff must be engaged as key stakeholders from the earliest stages of tool development, with their feedback incorporated through advisory boards and pilot testing to ensure usability and relevance. Seamless integration into existing workflows is essential, as tools that necessitate redundant data entry or force navigation across disconnected systems risk compounding workload rather than alleviating it. Moreover, training and transparency are equally vital, providing CRCs with a clear understanding of the algorithms’ inputs, outputs, and limitations.{17} This fosters trust, encourages informed use, and ensures facilitation of adoption. Most importantly, AI platforms must be supported by rigorous empirical validation; in the absence of such evaluation, claims of improved efficiency, reduced burden, and enhanced diversity will remain speculative.
The fidelity and ultimate utility of AI models remain inherently dependent on the quality of their input data.{18} Persistent systemic barriers, including fragmented electronic health record systems, entrenched data silos, and limited interoperability across healthcare platforms, continue to hinder effective operationalization.{19} Unless these foundational issues are addressed, even the most sophisticated AI applications will face restricted applicability. Progress will require coordinated efforts to improve data standardization, interoperability, and governance, thereby creating the infrastructure necessary for AI to achieve its full potential in clinical research.{20}
Summary of Guiding Principles
Effective AI integration in clinical research requires a coordinated approach across industry operations, workforce development, and policy. From an operational standpoint, organizations should prioritize site-centric design, developing AI tools in close collaboration with front-line research staff to ensure alignment with real-world workflows. AI should be viewed as a tool to reduce administrative burden and enhance efficiency, rather than an added layer of complexity, with pilot testing across diverse site types helping to identify barriers and refine implementation strategies.{21}
In parallel, a strong emphasis on workforce training and development is essential. Structured AI literacy programs, competency frameworks, and continuous learning opportunities can build technical confidence, ethical awareness, and adaptability among clinical research professionals.{22} At the policy level, collaboration among sponsors, regulators, and professional organizations is key to promoting transparency, interoperability, and equitable access to AI resources.{22,23} Upholding human oversight and ethical stewardship ensures that AI serves to augment, rather than replace, human expertise.{22,24} By embedding workforce readiness, collaboration, and ethical governance at the heart of innovation, the clinical research ecosystem can advance toward a future where AI meaningfully enhances both operational performance and the human dimensions of research. Table 3 outlines the major ethical and regulatory standards that govern AI data integrity and participant protection.
Table 3: Industry Recommendations—Strategic Actions for Effective AI Adoption in Clinical Research Operations
|
||||||||||||||||||||
Implications for Practice and Future Research
For AI adoption to be successful in clinical research, organizational leadership must prioritize capacity building, digital literacy, and cultural readiness. Institutions should embed continuous education on AI literacy within workforce development frameworks, ensuring that clinical research professionals understand both the capabilities and limitations of emerging tools. Collaborative learning networks between academic and community-based sites can promote knowledge exchange and harmonized standards.{7}
Future research should examine the longitudinal effects of AI integration on research quality, operational efficiency, and participant outcomes. Evaluating outcomes through a systems-thinking lens will help determine whether AI serves as a true facilitator of research excellence or simply adds another layer of technological complexity. The ultimate goal is to move from theoretical adoption models toward measurable, sustainable integration that enhances the integrity and inclusivity of clinical research.
Conclusion
The adoption of AI in clinical research represents both a technological and human transformation. A theory-driven, site-centric framework provides a pathway for understanding and addressing the barriers that impede AI literacy and utilization. By grounding practice in behavioral theory, embracing ethical and equitable implementation, and fostering site-level engagement, the research community can ensure that AI becomes a tool for empowerment rather than exclusion. Sustained progress will depend on bridging the gap between policy and practice, ensuring that innovation translates into tangible benefits for patients, professionals, and the broader healthcare ecosystem.
The path forward is therefore not solely technological but collaborative and human-centered, requiring the harmonization of innovation, workflow design, and workforce development. By empowering CRCs and CRAs through education, engagement, and inclusion in decision-making, the clinical research enterprise can unlock AI’s true potential: to reduce administrative burden, enhance trial quality, and build a sustainable and resilient research workforce prepared for the future of data-driven medicine.
Conflicts of Interest: None declared.
Funding: None.
References
- U.S. Food and Drug Administration. 2025. Considerations for the Use of Artificial Intelligence to Support Regulatory Decision-Making for Drug and Biological Products: Guidance for Industry and Other Interested Parties (Draft). https://www.fda.gov/media/184830/download
- Askin S, Burkhalter D, Calado G, El Dakrouni S. 2023. Artificial Intelligence Applied to Clinical Trials: Opportunities and Challenges. Health and Technology 13(2):203–13. https://doi.org/10.1007/s12553-023-00738-2
- Shah P, Kendall F, Khozin S, et al. 2019. Artificial Intelligence and Machine Learning in Clinical Development: A Translational Perspective. npj Digital Medicine 2(1):69. https://doi.org/10.1038/s41746-019-0148-3
- Hale GA, Pullum J. 2022. Clinical Research Organizations. In Pediatric Cancer Therapeutics Development, ed. by DiMartino J, Reaman GH, Smith FO. Springer International Publishing. https://doi.org/10.1007/978-3-031-06357-2_8
- Mora V, Colantuono S, Fanali C, et al. 2023. Clinical Research Coordinators: Key Components of an Efficient Clinical Trial Unit. Contemporary Clinical Trials Communications 32):101057. https://doi.org/10.1016/j.conctc.2023.101057
- Freel SA, Snyder DC, Bastarache K, et al. 2023. Now is the Time to Fix the Clinical Research Workforce Crisis. Clinical Trials 20(5):457–62. https://doi.org/10.1177/17407745231177885
- Marangunić N, Granić A. 2015. Technology Acceptance Model: A Literature Review from 1986 to 2013. Universal Access in the Information Society 14(1):81–95. https://doi.org/10.1007/s10209-014-0348-1
- Davis FD, Granić A. 2024. Revolution of TAM. In The Technology Acceptance Model: 30 Years of TAM, ed. by Davis FD, Granić A. Springer International Publishing. https://doi.org/10.1007/978-3-030-45274-2_3
- Venkatesh V, Davis FD. 2000. A Theoretical Extension of the Technology Acceptance Model: Four Longitudinal Field Studies. Management Science 46(2):186–204. https://www.jstor.org/journal/manascie
- Venkatesh V, Bala H. 2008. Technology Acceptance Model 3 and a Research Agenda on Interventions. Decision Sciences 39(2):273–315. https://doi.org/10.1111/j.1540-5915.2008.00192.x
- Lee AT, Ramasamy RK, Subbarao A. 2025. Understanding Psychosocial Barriers to Healthcare Technology Adoption: A Review of TAM Technology Acceptance Model and Unified Theory of Acceptance and Use of Technology and UTAUT Frameworks. Healthcare 13(3):250. https://doi.org/10.3390/healthcare13030250
- Chopra H, Annu, Shin DK, et al. 2023. Revolutionizing Clinical Trials: The Role of AI in Accelerating Medical Breakthroughs. International Journal of Surgery 109(12):4211–20. https://doi.org/10.1097/JS9.0000000000000705
- Ng DTK, Wu W, Leung JKL, Chiu TKF, Chu SKW. 2024. Design and Validation of the AI Literacy Questionnaire: The Affective, Behavioural, Cognitive and Ethical Approach. British Journal of Educational Technology 55(3):1082–104. https://doi.org/10.1111/bjet.13411
- Argyris A. 2020. Three Ways Site-Centric Solutions Streamline Study Execution. Clinical Researcher 34(9). https://acrpnet.org/2020/11/10/three-ways-site-centric-solutions-streamline-study-execution
- Senn C. 2024. From Isolation to Integration: Improving Site–Sponsor Collaboration in Clinical Trial Startup. Applied Clinical Trials. https://www.appliedclinicaltrialsonline.com/view/integration-improving-site-sponsor-collaboration-clinical-trial-startup
- Brathwaite JS, Rajasekaran N, Sheth M. 2025. Aligned for Impact: Strengthening Sponsor–CRO–Site Partnerships in Today’s Trials. Clinical Researcher 39(5). https://acrpnet.org/2025/10/21/aligned-for-impact-strengthening-sponsor-cro-site-partnerships-in-todays-trials
- Gazquéz-Garcia J, Sánchez-Bocanegra CL, Sevillano JL. 2025. AI in the Health Sector: Systematic Review of Key Skills for Future Health Professionals. JMIR Medical Education 11:e58161. https://doi.org/10.2196/58161
- Schwabe D, Becker K, Seyferth M, Klaß A, Schaeffter T. 2024. The METRIC-Framework for Assessing Data Quality for Trustworthy AI in Medicine: A Systematic Review. npj Digital Medicine 7(1):203. https://doi.org/10.1038/s41746-024-01196-4
- Torab-Miandoab A, Samad-Soltani T, Jodati A, Rezaei-Hachesu P. 2023. Interoperability of Heterogeneous Health Information Systems: A Systematic Literature Review. BMC Medical Informatics and Decision Making 23(1):18. https://doi.org/10.1186/s12911-023-02115-5
- Bouderhem R. 2024. Shaping the Future of AI in Healthcare through Ethics and Governance. Humanities and Social Sciences Communications 11(1):416. https://doi.org/10.1057/s41599-024-02894-w
- You JG, Hernandez-Boussard T, Pfeffer MA, et al. 2025. Clinical Trials Informed Framework for Real-World Clinical Implementation and Deployment of Artificial Intelligence Applications. npj Digital Medicine 8:107. https://doi.org/10.1038/s41746-025-01506-4
- Singh MP, Keche YN. 2025. Ethical Integration of Artificial Intelligence in Healthcare: Narrative Review of Global Challenges and Strategic Solutions. Cureus 17(5):e84804. https://doi.org/10.7759/cureus.84804
- Kim JY, Hasan A, Kueper J, Tang T, Hayes C, Fine B, Balu S, Sendak M. 2025. Establishing Organizational AI Governance in Healthcare: A Case Study in Canada. npj Digital Medicine 8(1):522. https://doi.org/10.1038/s41746-025-01909-3
- Daneshvar N, Pandita D, Erickson S, Sulmasy LS, DeCamp M (for the ACP Medical Informatics Committee and the Ethics, Professionalism and Human Rights Committee). 2024. Artificial Intelligence in the Provision of Health Care: An American College of Physicians Policy Position Paper. Annals of Internal Medicine 177(7). https://doi.org/10.7326/M24-0146
- Nair M, Svedberg P, Larsson I, Nygren JM. 2024. A Comprehensive Overview of Barriers and Strategies for AI Implementation in Healthcare: Mixed-Method Design. PLOS ONE 19(8):e0305949. https://doi.org/10.1371/journal.pone.0305949

Justin Scott Brathwaite, MBA, PMP, is a Clinical Research Associate at Fortrea, a PhD student in Clinical Research at the University of Jamestown, and an Editorial Advisor for ACRP’s Clinical Researcher journal. He has five years of experience in study start-up operations and is a two-time finalist in the PharmaTimes Clinical Researcher of the Year (Study Start-Up category) competition.

Syed A. A. Rizvi, MD, PhD(Pharm), PhD(Chem), MPH, MBA, MS, MSN, MSc, BSc, BSN, CCRN, CEN, CMRN, TNS, VA-BC, LSSBB, FRSM, is a physician-scientist, educator, and healthcare leader with more than 27 years of experience spanning clinical research, pharmaceutical sciences, drug development, regulatory affairs, medical writing, translational medicine, patient care, and medical education. He currently serves as Professor at Larkin University and Adjunct Faculty at the University of Jamestown. Dr. Rizvi has authored more than 300 scholarly publications, including journal articles, books, and book chapters and has contributed to more than 470 editorial and peer-review activities across the biomedical and pharmaceutical sciences. His work focuses on advancing pharmaceutical innovation, clinical research, translational medicine, healthcare education, and evidence-based practice through interdisciplinary collaboration and academic leadership.


