
Clinical Researcher—August 2020 (Volume 34, Issue 7)
QUALITY CONCERNS
Patrick Hughes
Risk-based quality management (RBQM) is a system for managing quality throughout a clinical trial. The data-driven elements of this type of strategy have evolved substantially over the past few years, as an extension to the original principles underpinning risk-based monitoring (RBM). This article will outline the difference between RBM and RBQM, highlighting some of the advantages and benefits of managing all areas of quality in a clinical trial. It will also provide a discussion of the implementation of the method alongside some of the challenges related to embracing the change. It will outline how sponsors and contract research organizations (CROs) can harness the power of risk-based trial management, making clinical trials better, faster, and cheaper for the industry and safer for patients.
A Need for Change
From the year 2000, a continual increase in the complexity of clinical trial designs, highly publicized safety issues with marketed drugs, and a slowing of innovation coupled with patent expirations saw the cost and duration of clinical development steadily increase, while profit margins dwindled. While the previous decade had been a time of relative economic health for the biopharmaceutical industry, at the turn of the century drug makers found themselves faced with growing pressure from multiple directions.
Between 2000 and 2012, a review of marketing submissions to the U.S. Food and Drug Administration revealed that about one-third (32%) of all first-cycle review failures, or 16% of submissions overall, were driven by quality issues.{1} The increasing complexity of trials means they take longer and cost more. This dynamic also adds significant risk to the operational success of research, both in terms of recruiting and retaining patients, and in generating the reliable results needed to support ultimate marketing approvals. It is apparent that the traditional way of conducting trials is not fit for the 21st century.
Understanding RBM
RBM, which is most efficiently achieved by sponsors harnessing technology and real-time information to proactively monitor risk, was written into U.S. and European regulatory guidance in 2013. In its simplest form, RBM strategies use software, data inputs, and analytics to monitor risk and support critical thinking and decision making. By giving sponsors the ability to identify and correct issues as and when they arise, RBM can improve data quality and patient safety as well as reduce costs.
At its core, RBM is the operational analogue to the tenets of “quality by design” (QbD). Both models have the same fundamental goal of improving the operational success rate of clinical research through higher quality, shorter timelines, and greater efficiency. QbD and RBM are also linked by methodology, as they both call for ongoing assessment and mitigation of operational risk.
Embracing RBQM
RBQM methodology is a very timely development that sponsors and CROs are now embracing to address the growing crisis in research complexity, duration, and cost. The latest version of the Good Clinical Practice (GCP) quality standard extends the RBM approach to every aspect of study execution, applying the principles to all areas of quality management. The ICH E6(R2) guideline for GCP from the International Council for Harmonization outlines the driving factors of this approach, including the transition away from largely paper-based research to the modern approach of electronic and digital technologies including electronic data capture, electronic clinical outcome assessment, and interactive response technology. This has opened a tremendous opportunity to plan and manage clinical research more effectively and efficiently.
RBQM implementation can be overwhelming for an organization, given the wealth of information that is currently available. Starting simple is the way to maintain focus and concentrate on the elements of RBQM that are most important to gain immediate quick wins and success in the long term. The key to success is to apply thoughtful but simple processes, smart technology, and a focus on evolutionary change management.
Making the Transition
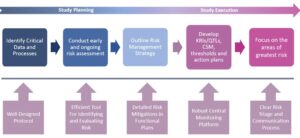
RBQM encompasses all elements of the study, from planning right through to execution. Risk management underpins the overall quality of the trial by identifying, controlling, and communicating. ICH E6(R2) sets out what a gold standard RBQM system should cover:
- Critical process and data identification
- Risk identifications
- Risk evaluation
- Risk control
- Risk communication
- Risk review
- Risk reporting
Further, centralized statistical monitoring (CSM) is a critical component of the operational success of RBQM, as it is a key and under-used weapon for quality oversight. CSM lies at the heart of RBQM (see Figure 1). It interrogates all clinical and key operational data to find anomalies and discrepancies that would remain undetected by traditional techniques. It is more than just computing statistics on a subset of key variables—it is about processing all data and guiding users to where the potential issues might lie, or a “boil the ocean” approach to risk identification and mitigation.
Figure 1: Centralized Statistical Monitoring Model
An effective centralized monitoring approach should include the following three components:
- Data surveillance
- Key risk indicators (KRIs)
- Quality tolerance limits (QTLs)
When it comes to KRIs and QTLs, quality is much more important than quantity. Sponsors and CROs should identify a core set (10 to 15) of appropriate KRIs and focus on ensuring that these are optimized to detect risk as early as possible and minimize likelihood of false alerting.
The same principle should apply to QTLs (four or five), which should focus on the most important study-level risks, or “failure points.” Data surveillance, which is sometimes referred to as CSM, has been under-appreciated and under-utilized by many organizations, but provides an effective independent and objective quality oversight process.
While KRIs and QTLs are designed to monitor for pre-identified areas of risk, data surveillance or CSM can expose forms of study abnormality and misconduct that may be difficult to identify and/or characterize during pre-study risk planning. By running a comprehensive set of well-designed statistical tests across a broad swath of study data, the method can spot atypical patterns that represent potential intentional or non-intentional misconduct. It can flag issues such as fraud, sloppiness, or training needs, as well as malfunctioning or poorly calibrated study equipment.
Elements to Success
RBQM relies on a combination of different tools. A central monitoring platform can act as the enabling technology, encompassing central data review, risk assessment, KRIs, data quality oversight, and issue and action tracking management modules. None of the key components of RBQM implementation, including pre-study risk planning, adaptive/dynamic site monitoring with a significant reduction in source data verification, and centralized monitoring, need to be complex to be effective. Risk findings should be documented thoroughly and accurately for regulatory inspection purposes. A plan should ideally cover the overall objectives, proactive data monitoring, and communication.
The first step in proactive data monitoring is to identify what is possible to mitigate, eliminate, and accept. This all forms part of various plans, including those for data, training, monitoring, statistical analysis, safety, medical monitoring, quality, and other functional plans. KRIs, QTLs, CSM, and risk communication are all crucial to the process to identify risk signals and comply with the regulatory obligations. The entire study team should be aware of the risks and how they are being managed.
Although the many layers of the model may seem daunting at first, sustainable success in adopting RBQM begins with establishing and confirming the primary objectives for adopting the strategy (i.e., what is the organization trying to achieve with RBQM?).
Each of the following three dimensions of value should be considered:
- Improved quality
- Reduced operational costs
- Shorter timelines
Moving Forward
Improving data quality and patient safety, while controlling the spiralling costs of drug development research, were the primary objectives behind the shift toward RBM over the last eight years. The model’s success, combined with advances in clinical trial technology, has seen the approach extended to cover the whole of trial execution in a methodology widely referred to as RBQM. Elements of RBQM can be implemented individually and independently to great success, making clinical trials better, faster, and cheaper for sponsors and CROs and safer for patients.
Reference
1. https://jama.jamanetwork.com/article.aspx?articleid=1817795

Patrick Hughes is Co-founder and Chief Commercial Officer of CluePoints.


